Health Information Exchange: What It Is And How It Works

You've probably heard the term thrown around in vendor pitches, compliance meetings, or EHR onboarding docs, but nobody stopped to explain it. What is health information exchange, exactly, and why does every serious healthcare app seem to depend on it? If you're building or buying healthcare technology, you need a real answer, not marketing language.
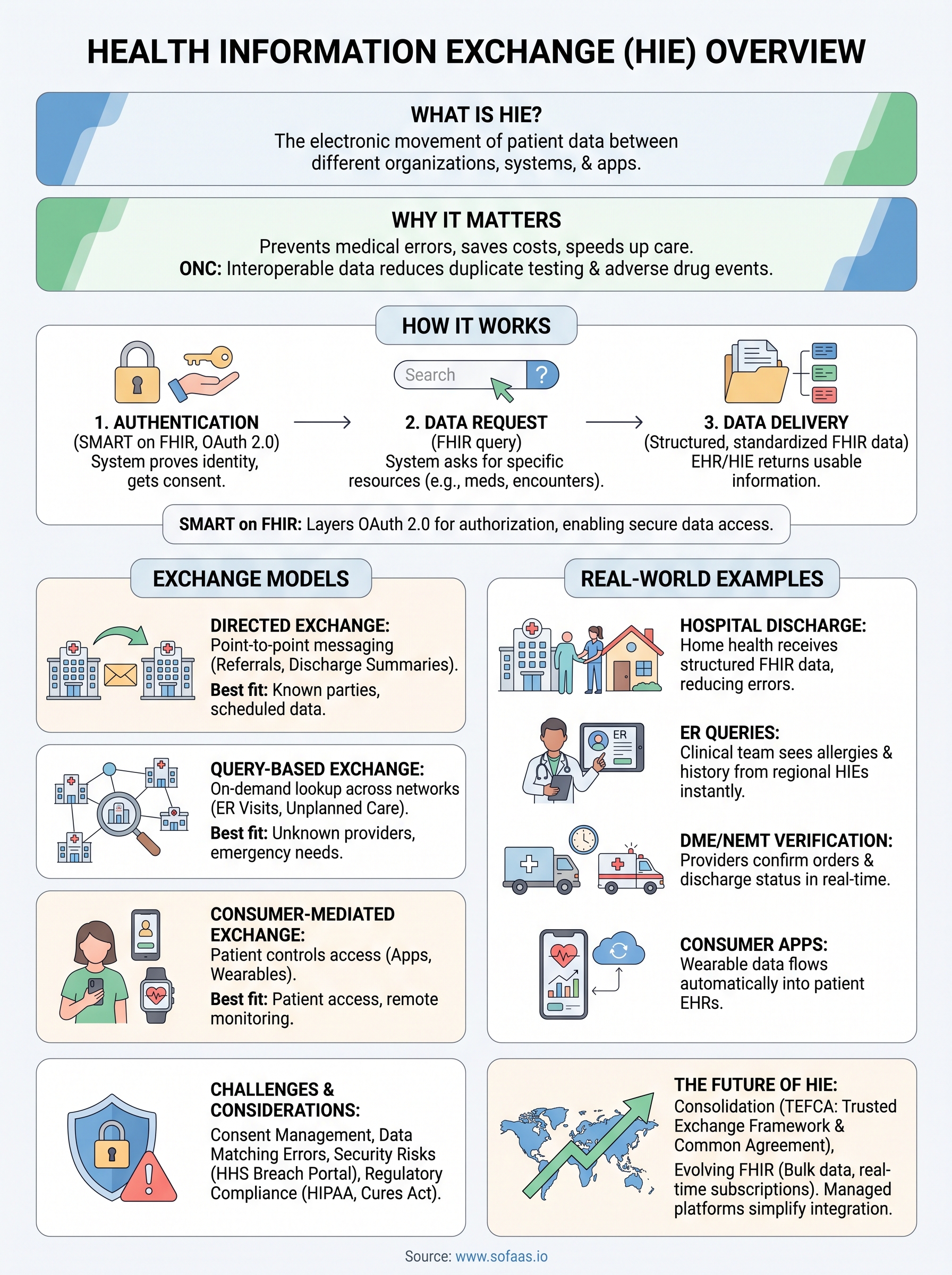
Health information exchange, or HIE, is the electronic movement of patient data between different healthcare organizations, systems, and applications, so the right information shows up where and when it's needed. It covers everything from a hospital sending discharge summaries to a primary care doctor, to an app pulling lab results directly from an EHR. Understanding how HIE works matters because it directly shapes how fast you can build, how compliant you stay, and how much friction patients and providers experience.
In this article, we'll break down the different types of health information exchange, walk through the technical mechanics behind it, including standards like SMART on FHIR, and explain why it's become foundational to modern healthcare interoperability. By the end, you'll know exactly where HIE fits into your own integration strategy.
Why health information exchange matters in healthcare
Health information exchange matters because fragmented patient data kills people, wastes money, and slows down every healthcare business trying to move fast. Before HIE became standard practice, a patient's history lived in a dozen disconnected silos: one hospital's EHR, a specialist's paper chart, a pharmacy database, a home health agency's spreadsheet. Nobody had the full picture. Fragmented records force clinicians to guess, repeat tests, and miss allergies or medication conflicts that were sitting in a system they simply couldn't see.
The clinical cost of disconnected data
When a patient shows up in an emergency room unconscious, the ER team needs their medication list, allergies, and recent labs immediately, not after a fax request to three different offices. Health information exchange closes that gap by letting authorized systems pull that data electronically, often in seconds. The Office of the National Coordinator for Health Information Technology has documented how interoperable data sharing reduces duplicate testing and adverse drug events, two of the most preventable and costly problems in American healthcare. You can read more about ONC's interoperability work directly on HealthIT.gov.
Every duplicate test, missed allergy alert, or delayed referral traces back to a health information exchange gap that didn't get closed.
Why it matters for the businesses building healthcare technology
If you're a DME provider, home health agency, NEMT company, or software vendor building tools for any of these groups, HIE isn't an abstract policy issue. It's the mechanism that determines whether your application can actually function in a real clinical workflow. A remote patient monitoring app that can't pull vitals into the patient's EHR is a dead end for adoption. A NEMT platform that can't verify a patient's discharge status in real time can't schedule rides efficiently. HIE is the plumbing that makes these use cases possible at all.
Here's a quick look at what changes when HIE is actually working versus when it isn't:
| Without HIE | With HIE |
|---|---|
| Manual faxing and phone calls between providers | Automated electronic data exchange |
| Duplicate labs and imaging | Shared results across care settings |
| Delayed care coordination | Near real-time updates between systems |
| High risk of medication errors | Full medication history visible to all providers |
| Slow onboarding for new health tech apps | Faster integration through standardized data formats |
Regulatory pressure is only increasing
Regulators aren't waiting around for the industry to catch up on its own. The 21st Century Cures Act and the ONC's information blocking rules now require most healthcare providers and technology vendors to support electronic access to patient data, and penalties for noncompliance are real. Interoperability requirements have moved from a competitive advantage to a baseline expectation, especially for anyone selling into hospitals, health systems, or payers. If your application can't participate in health information exchange, you're not just missing a feature, you're potentially locked out of contracts entirely.
This is also why the question of what is health information exchange comes up so often in vendor evaluations and RFPs. Procurement teams at hospitals and health systems now ask directly how a product handles data exchange, because they've been burned by systems that create more silos instead of closing them. Getting this right isn't optional anymore, it's the price of entry for building healthcare technology that actually gets adopted and scales beyond a pilot program.
How health information exchange works
Underneath the marketing language, health information exchange runs on a fairly specific technical stack: standardized data formats, secure transport protocols, and agreed-upon rules for who can access what. Data standardization is the foundation. Before HL7 and FHIR became common, every EHR vendor stored patient data in its own proprietary format, which meant every integration was a custom, expensive project. FHIR (Fast Healthcare Interoperability Resources) changed that by giving the industry a shared, structured way to represent things like patient demographics, lab results, and medications as discoverable API resources.

The three-step flow of an exchange
Most health information exchange follows the same basic pattern, whether it's a hospital pulling records or an app requesting lab data. Here's what that flow typically looks like:
- Authentication and authorization: The requesting system proves its identity and gets patient or provider consent, usually through an OAuth 2.0 flow built on the SMART on FHIR framework.
- Data request: The system queries a FHIR-enabled endpoint for specific resources, like a patient's medication list or recent encounters.
- Data delivery: The EHR or health information exchange network returns structured, standardized data that the requesting application can immediately use, without manual reformatting.
Without standardized authorization and data formats, health information exchange collapses back into faxes and phone calls.
Why SMART on FHIR became the connective tissue
SMART on FHIR matters here because it solves the two hardest parts of this process: securely authenticating a user and structuring the data consistently once you have access. It layers OAuth 2.0 authorization on top of the FHIR standard, so a third-party app can request exactly the scope of data it needs, get explicit patient or provider consent, and then pull that data in a format that looks the same whether it's coming from Epic, Cerner, or Allscripts. That consistency is what lets a developer build one integration instead of ten.
This is also where a lot of otherwise capable engineering teams get stuck. Handling token refreshes, consent revocation, audit logging, and EHR-specific quirks in FHIR implementations takes real specialized effort, and getting any of it wrong creates compliance risk. Managed integration platforms exist specifically to absorb that complexity, so your team can focus on the application logic instead of rebuilding OAuth flows and connector maintenance for every EHR you need to support.
Types of health information exchange models
Health information exchange isn't a single architecture. Three distinct models have emerged over the past two decades, each solving the data-sharing problem differently, and each with tradeoffs that matter depending on your use case. Directed exchange is the simplest: two known parties send patient data directly to each other, like a hospital sending a referral packet to a specialist. It's essentially secure, structured messaging, often built on standards like Direct Secure Messaging, and it works well when you already know exactly who needs the data and when.

Query-based exchange
Query-based exchange flips the model. Instead of pushing data to a known recipient, a provider or application searches for patient information across participating systems on demand, typically during an unplanned encounter like an ER visit. This is where regional and state HIEs play a major role, aggregating data from multiple hospitals and clinics so a provider can pull up a patient's history even if that patient has never been seen at their facility before. The tradeoff is complexity: query-based networks require significant governance, data-matching logic, and participation agreements among competing organizations.
Consumer-mediated exchange
Consumer-mediated exchange puts the patient in the driver's seat. Here, the individual controls access to their own records and decides which apps or providers can pull data, usually through a patient portal or a SMART on FHIR-enabled app. This model has grown fastest since the Cures Act mandated patient access to their own electronic health information, and it's the model most relevant to app developers building consumer-facing health tools.
The exchange model you build against determines whether your integration takes days or months to get right.
Comparing the three models
| Model | How it works | Best fit |
|---|---|---|
| Directed exchange | Point-to-point messaging between known parties | Referrals, discharge summaries |
| Query-based exchange | On-demand lookup across a network | Emergency care, care coordination |
| Consumer-mediated exchange | Patient authorizes and controls access | Patient apps, remote monitoring, wearables |
Most real-world healthcare technology stacks end up touching more than one of these models simultaneously. A home health agency might receive a directed referral, query a regional HIE for medication history, and then connect to a patient's EHR through a consumer-mediated SMART on FHIR flow, all for the same patient. Knowing which model you're working with at each step keeps your integration scoped correctly instead of trying to force one architecture to solve every problem.
Health information exchange in action: real-world examples
Theory only gets you so far. Seeing how health information exchange plays out in actual clinical and operational settings makes the concept concrete, especially if you're building or buying software for one of these workflows yourself.

Hospital discharge to home health handoff
When a hospital discharges a patient who needs ongoing care, a home health agency typically receives a referral packet through directed exchange, containing the discharge summary, medication list, and physician orders. Without electronic exchange, that packet arrives by fax, often incomplete, and someone on the agency side has to manually re-enter everything into their own system. With HIE in place, the agency's software pulls structured FHIR data directly, cutting intake time from hours to minutes and reducing transcription errors that lead to missed medications or wrong dosages.
Emergency departments querying regional networks
A patient arrives unconscious at an ER with no ID and no known history. The clinical team queries a regional health information exchange, which aggregates records from every participating hospital and clinic in the area. Within seconds, they can see prior allergies, chronic conditions, and recent imaging, even though the patient has never set foot in that specific ER before. This is query-based exchange doing exactly what it was designed for: filling a gap when there's no existing relationship between provider and patient.
The value of health information exchange is easiest to see in the moments when there's no time to ask questions and no one to call.
DME and NEMT providers verifying eligibility in real time
DME providers and NEMT companies depend on accurate, current data to do their jobs at all. A durable medical equipment supplier needs to confirm a physician's order and diagnosis code before shipping equipment. An NEMT provider needs to know a patient's discharge time and destination to schedule a ride without delay. Both scenarios rely on real-time exchange with the referring provider's EHR, and both fail badly when that data arrives late or not at all.
Consumer apps syncing wearable and remote monitoring data
A remote patient monitoring app collecting blood pressure or glucose readings from a wearable device needs that data to land inside the patient's actual medical record, not just a standalone dashboard nobody at the clinic ever opens. Consumer-mediated exchange, through a SMART on FHIR authorization flow, lets the patient approve that connection once and have readings flow automatically into their EHR going forward, giving their care team visibility without extra manual work on either side.
Key challenges and privacy considerations
Health information exchange solves real problems, but it creates new ones too, and pretending otherwise sets up a rough surprise later. Patient consent and data matching cause the most friction in practice. Matching the right records to the right patient across systems that use different identifiers, spellings, and formats is genuinely hard, and a mismatch means the wrong medication history shows up for the wrong person. That's not a minor bug, it's a patient safety issue with legal consequences attached.
Security exposure grows with every connection
Every new integration point is another potential attack surface. Breach exposure increases as more systems exchange more data, and healthcare remains one of the most targeted industries for ransomware and data theft precisely because patient records are valuable on the black market. The U.S. Department of Health and Human Services tracks breach reports affecting healthcare organizations, and the numbers climb almost every year, which you can verify through the HHS Office for Civil Rights breach portal. Encryption, audit logging, and strict access controls aren't optional extras here, they're the baseline cost of participating in exchange at all.
A single unencrypted connection can undo years of trust built through compliant, well-governed data exchange.
Regulatory compliance is a moving target
HIPAA sets the floor, but information blocking rules under the 21st Century Cures Act add another layer of obligation on top of it, requiring most providers and vendors to make patient data available electronically unless a specific exception applies. Keeping up with these rules while also managing consent revocation, minimum necessary access, and state-level privacy laws demands ongoing legal and technical attention, not a one-time compliance checklist.
The tradeoffs teams actually face
Here's what most teams run into when they start exchanging data at scale:
- Consent management complexity: tracking who authorized what, and for how long, across multiple apps and providers.
- Identity resolution errors: duplicate or mismatched patient records causing incomplete or incorrect data views.
- Audit trail requirements: proving, after the fact, exactly who accessed what data and why.
- Vendor risk: every EHR connector or third-party API adds a dependency that needs its own security review.
None of these challenges are reasons to avoid health information exchange. They're reasons to build or buy infrastructure that treats compliance and security as part of the architecture, not an afterthought bolted on once something breaks.
How developers connect applications to HIE and EHR data
Building the actual connection between your application and a health information exchange or EHR looks straightforward on a whiteboard and gets messy fast in practice. Developer access typically starts with registering your app with each EHR vendor's developer program, then working through their specific SMART on FHIR implementation, which varies more than the standard implies. Epic, Cerner, and Allscripts each have their own quirks in how they handle scopes, token lifetimes, and sandbox environments, so "standardized" doesn't mean "identical."
The typical build-it-yourself path
Going the manual route means your team owns every piece of this process, and each piece takes real engineering time:
- Register as a developer with each EHR vendor and request production access, a process that can take weeks per vendor.
- Build and test OAuth 2.0 authorization flows against each vendor's sandbox, handling scopes, refresh tokens, and consent screens.
- Map FHIR resources correctly, since implementation details differ slightly between vendors even for the same resource type.
- Stand up HIPAA-compliant infrastructure for audit logging, encryption, and access controls before you can even request production credentials.
- Maintain all of it going forward as EHR vendors push updates, deprecate endpoints, and change certification requirements.
Every EHR connector you build in-house is another system your team owns for the life of the product, not just for launch day.
Why most teams end up choosing a managed layer
That maintenance burden is exactly why managed integration platforms exist. Instead of building and re-building separate connectors for Epic, Cerner, and Allscripts, a platform like SoFaaS gives you a single unified API that handles authorization, token refresh, and FHIR resource mapping consistently across EHRs. Your team requests the data it needs, and the platform absorbs the vendor-specific complexity underneath.
This matters most when you're trying to move fast without cutting corners on compliance. A no-code connection workflow backed by SOC 2 Type II infrastructure means your engineers spend their time on the actual product, not on debugging why Cerner's token expiration behaves differently than Epic's. For a DME provider, home health agency, or health tech startup trying to launch in weeks rather than quarters, that difference in build time often decides whether the project ships at all.
The future of health information exchange
Health information exchange is heading toward consolidation, not more fragmentation. National-level frameworks are replacing the patchwork of regional and state HIEs that don't talk to each other, and that shift changes how you should plan integrations over the next few years. If you're building on today's exchange landscape, you're building on the early version of something that's about to get a lot more standardized.
TEFCA and the push toward one network
The Trusted Exchange Framework and Common Agreement (TEFCA), run through the ONC, aims to connect every qualified health information network into a single interoperable system, so a query in one region can reach data anywhere in the country. You can read the technical framework directly on HealthIT.gov. Instead of negotiating separate participation agreements with a dozen regional HIEs, organizations that join TEFCA get one legal and technical pathway to nationwide exchange.
The winners in health information exchange won't be the ones with the most connectors, they'll be the ones ready when the connectors consolidate into one network.
FHIR keeps maturing past basic data retrieval
FHIR implementations are moving beyond simple read access toward richer use cases: bulk data export for population health, subscription-based real-time notifications instead of polling, and standardized clinical decision support hooks. That means the SMART on FHIR foundation you build on today gets more capable without requiring you to rip out your integration and start over, as long as you built on standards rather than custom workarounds.
What this means if you're building now
Here's the practical takeaway for anyone architecting a healthcare application today:
- Build on standards, not shortcuts. Custom, vendor-specific workarounds age poorly as TEFCA and FHIR evolve.
- Expect consolidation. Fewer, larger networks will replace today's fragmented regional patchwork.
- Plan for scale early. Bulk data and real-time subscriptions will matter more as adoption grows.
Teams that lean on a managed integration layer absorb these shifts automatically, since the platform updates underneath them, while teams maintaining custom connectors have to track every framework change themselves.
Bringing it all together
Health information exchange isn't a buzzword you can skip past anymore. It's the mechanism that decides whether patient data reaches the right system at the right moment, and whether your application actually works inside real clinical workflows. Understanding HIE means understanding directed, query-based, and consumer-mediated models, the SMART on FHIR standards underneath them, and the compliance obligations that come with every connection you build.
None of that has to slow you down. The teams that ship fastest aren't the ones avoiding this complexity, they're the ones handing it to infrastructure built specifically for it. Managed integration platforms exist so your engineers build product features instead of rebuilding OAuth flows for every EHR vendor.
If you're ready to connect your application to Epic, Cerner, or Allscripts without spending months on custom integration work, launch your SMART on FHIR app in a couple of steps and see how much faster this gets with the right platform underneath you.
The Future of Patient Logistics
Exploring the future of all things related to patient logistics, technology and how AI is going to re-shape the way we deliver care.
Thank you! Your submission has been received!
Oops! Something went wrong while submitting the form.