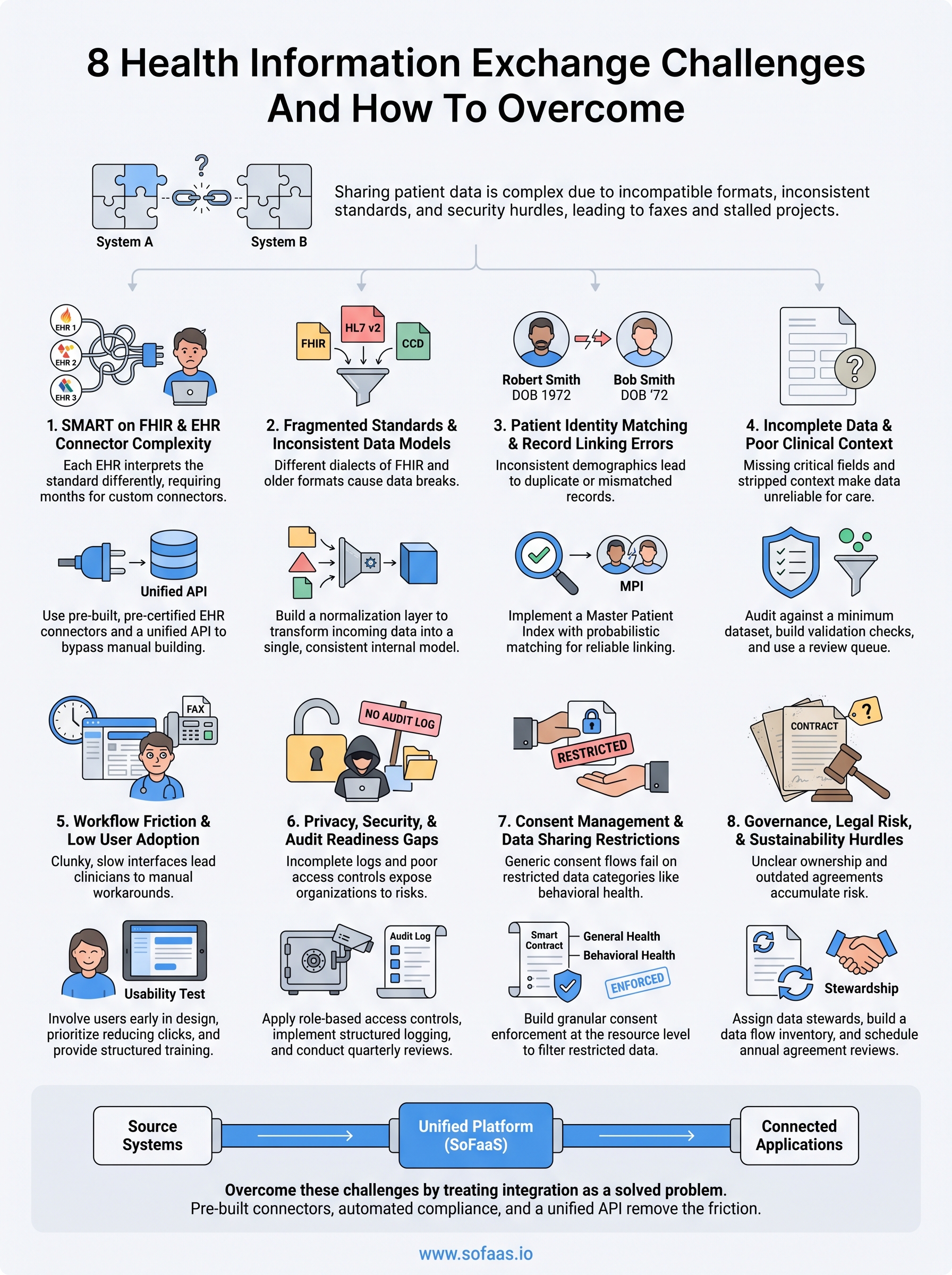
8 Health Information Exchange Challenges And How To Overcome

Sharing patient data between systems sounds straightforward, until you actually try to do it. Health information exchange challenges range from incompatible data formats and inconsistent standards to regulatory minefields and organizational resistance. These aren't theoretical problems. They're the reason clinicians still fax records, developers burn months on integration work, and healthcare organizations struggle to deliver coordinated care.
The push toward interoperability has made real progress over the past decade, thanks in part to standards like FHIR and frameworks like SMART on FHIR. But adopting those standards is only one piece of the puzzle. Security requirements, consent management, EHR variability, and the sheer cost of building compliant infrastructure continue to slow things down. For teams building health tech products, these barriers can stall a launch or drain engineering resources before the application even reaches patients.
At SoFaaS, we built a managed platform specifically to remove the integration burden from healthcare developers, pre-built EHR connectors, automated compliance, and a unified API that handles the complexity so your team doesn't have to. We see these challenges up close every day, and that perspective shapes what follows.
This article breaks down eight core challenges in health information exchange and offers practical strategies to address each one. Whether you're a CTO planning your integration roadmap or a product manager scoping your next build, you'll walk away with a clear picture of what's actually hard, and what you can do about it.
1. SMART on FHIR and EHR connector complexity
SMART on FHIR is the standard for connecting healthcare applications to EHRs, but implementing it from scratch is one of the most persistent health information exchange challenges teams face. Each EHR vendor interprets the standard differently, and building even a single reliable connector demands months of developer time, testing, and ongoing maintenance.
What this challenge looks like
Your team sets out to integrate with Epic or Cerner and quickly discovers that each EHR has its own quirks: different OAuth flows, proprietary endpoint structures, inconsistent FHIR resource support, and sandbox environments that don't accurately reflect production behavior. What looks like a two-week task in your sprint plan turns into a multi-month project with no clear end in sight.
The average healthcare integration project takes six to twelve months when built entirely in-house, with a significant portion of that time spent debugging EHR-specific edge cases.
Why it happens
FHIR defines a framework, not a finished product. EHR vendors have discretion over which resources they expose, how they handle authentication, and what extensions they support. This means there is no single SMART on FHIR implementation that works universally across Epic, Cerner, Allscripts, and others. Every connector is essentially a custom engineering project, and the knowledge required to build one correctly is narrow and in high demand.
How to overcome it
The most effective approach is to avoid rebuilding this infrastructure entirely. Use pre-certified EHR connectors wherever possible, and invest your engineering resources in the application logic that differentiates your product. If you must build connectors in-house, start by thoroughly reviewing each EHR's developer documentation and allocating time specifically for certification processes, which vary by vendor and can add weeks to your timeline.
How SoFaaS helps
SoFaaS provides pre-built connectors for major EHR systems including Epic, Cerner, and Allscripts, all accessible through a single unified API. Your team skips the connector-building phase entirely and moves directly to application development. Automated OAuth and token management are handled by the platform, removing one of the most error-prone parts of the integration process.
Metrics to track
Monitor these indicators to keep connector complexity from stalling your project:
- Time to first successful API call in a new EHR sandbox environment
- Integration failure rate across active EHR connections
- Token refresh error frequency as a proxy for OAuth stability
- Developer hours spent on connector maintenance per quarter
2. Fragmented standards and inconsistent data models
Even when two systems both claim to support FHIR, they often speak completely different dialects of the same specification. Fragmented standards and inconsistent data models are a core layer of health information exchange challenges that stay hidden until your integration breaks in a live environment.
What this challenge looks like
You request a patient's medication list from one EHR and receive a clean FHIR MedicationRequest bundle. The next system returns a proprietary format with custom extensions your parser doesn't recognize. Across different EHRs, the same clinical concept, a diagnosis, a lab result, or an allergy, can appear in entirely different structures, using code sets like ICD-10, SNOMED CT, or LOINC applied inconsistently or not at all.
Why it happens
FHIR defines a flexible specification, not a rigid schema. Vendors have significant latitude over which resources they expose, which extensions they add, and which terminologies they map to. Many older systems still rely on HL7 v2 or CCD/C-CDA formats that predate FHIR entirely, meaning your pipeline needs to handle multiple generations of data standards simultaneously.
How to overcome it
Build a normalization layer into your integration pipeline that transforms all incoming data into a consistent internal model before your application logic processes it. Standardize on a single canonical terminology like LOINC or SNOMED CT internally, and map every incoming code to that standard at the point of ingestion.
The more EHR sources you connect, the more critical a unified data model becomes to your application's reliability.
Metrics to track
Track these figures to surface data model problems before they reach users:
- Terminology mapping coverage across active EHR connections
- Parsing error rate broken down by source system
- Data normalization failure rate per integration endpoint
3. Patient identity matching and record linking errors
Patient identity matching sits at the core of many health information exchange challenges that teams don't anticipate until records start ending up in the wrong charts. When your system can't reliably determine that two records belong to the same patient, every downstream clinical decision built on that data becomes unreliable.
What this challenge looks like
Your integration pulls patient records from two separate EHRs and returns duplicate or mismatched profiles. One system stores "Robert Smith, DOB 1972-03-14" while another has "Bob Smith, DOB 03/14/72." Without a reliable matching layer, your application either creates duplicate records or worse, merges records for two different people entirely.
Patient misidentification contributes to serious safety events in hospitals, making accurate record linking one of the highest-stakes problems in health data exchange.
Why it happens
No universal patient identifier exists in the United States. Each EHR assigns its own internal patient ID, and demographic data like names, dates of birth, and addresses gets entered inconsistently across systems. Typographical errors, legal name changes, and data entry shortcuts compound the problem at scale.
How to overcome it
Implement a Master Patient Index (MPI) that uses probabilistic matching algorithms to compare multiple demographic fields simultaneously rather than relying on exact string matches. Combine name, date of birth, address, and phone number as weighted matching criteria, and build a manual review queue for records that fall into a low-confidence zone.
Metrics to track
- Duplicate record rate across linked sources
- Match confidence score distribution across your patient population
- False merge rate identified through clinical review
- Unlinked record percentage per active EHR connection
4. Incomplete data and poor clinical context
Receiving patient data is only half the problem. Even when records arrive without parsing errors or identity mismatches, missing fields and stripped clinical context can make that data nearly useless for care decisions. This is one of the subtler health information exchange challenges because your integration appears to be working correctly, yet the output still fails the clinicians relying on it.
What this challenge looks like
Your application pulls a patient's discharge summary and receives a FHIR document missing key fields like medication dosages, allergy severity, or the reason for a prior hospitalization. In other cases, coded values arrive without accompanying narrative notes, leaving clinicians with a data point but no clinical story behind it.
Incomplete records are frequently more dangerous than no record at all, because they create a false sense of completeness in your system.
Why it happens
Source systems were not designed with data sharing as a priority. Many EHR fields are optional, and clinicians under time pressure routinely skip them. Data also gets lost during format conversion between HL7 v2, CDA, and FHIR, where certain fields have no direct mapping and get silently dropped in translation rather than flagged for review.
How to overcome it
Audit your incoming data regularly against a defined minimum dataset that your application requires to function safely. Build validation checks at the point of ingestion that flag records with critical missing fields before they reach your clinical workflows, and route incomplete records to a human review queue rather than passing them through automatically.
Metrics to track
- Required field completeness rate per source EHR
- Records flagged for missing critical data per day
- Data loss rate during format conversion between standards
5. Workflow friction and low user adoption
Even technically sound integrations fail when the people using them reject them. Workflow friction is one of the most overlooked health information exchange challenges because it doesn't show up in your error logs. It shows up in adoption metrics, and by then the damage is already done.
What this challenge looks like
Your integration goes live and the data flows correctly, but clinicians keep defaulting to manual workarounds like phone calls, faxes, or printed summaries. Front-end staff find the new interface disruptive to their existing routines, and utilization numbers plateau well below target within the first few weeks.
Low adoption rates are often misread as a technology problem when they are actually a design and change management problem.
Why it happens
Healthcare workers operate under significant time pressure, and any new system that adds steps to their workflow will face resistance. Integration tools built primarily by engineers often optimize for technical correctness rather than clinical usability, producing interfaces that are accurate but slow and counterintuitive in practice.
Front-end staff typically have no input during the technical build phase, which means the integration lands in their workflow without accounting for how they actually work. The result is a system that functions correctly on paper but creates friction at every touchpoint they interact with daily.
How to overcome it
Involve end users early in the design process, before your integration is built, not after. Run structured usability tests with actual clinicians and front-end staff, and prioritize reducing clicks and context switches over adding features. Designated workflow champions and structured onboarding training significantly improve adoption rates once you go live.
Metrics to track
- Daily active users as a percentage of total licensed users
- Manual workaround frequency reported through staff feedback
- Task completion time for common clinical workflows
- Feature utilization rate across your integration touchpoints
6. Privacy, security, and audit readiness gaps
Security failures in health data exchange carry consequences far beyond a technical incident. Among the most costly health information exchange challenges, privacy and audit gaps expose your organization to HIPAA penalties, breach notification obligations, and reputational damage that take years to recover from.

What this challenge looks like
Your integration moves patient data between systems, but audit logs are incomplete, access controls are inconsistently applied, and your team can't produce a clean record of who accessed what data and when. During a compliance review or security incident, that gap becomes an immediate liability.
Incomplete audit trails are one of the most common findings in HIPAA enforcement actions, and regulators treat them as evidence of systemic negligence rather than isolated oversights.
Why it happens
Most integration pipelines are built for functionality first, with security and logging added later as an afterthought. Teams moving fast to hit a launch deadline frequently skip end-to-end encryption, row-level access controls, and structured audit event capture. When those gaps compound across multiple EHR connections, your attack surface grows faster than your visibility into it.
How to overcome it
Apply role-based access controls at the API layer from day one, not after your first security review. Implement structured audit logging that captures every data access event with a timestamp, user identity, and resource identifier. Schedule quarterly security reviews against your HIPAA obligations and maintain documentation that maps every data flow in your integration architecture.
Metrics to track
- Audit log coverage rate across all active data access events
- Mean time to detect unauthorized data access attempts
- Encryption coverage across data in transit and at rest
- Open security findings per quarterly review cycle
7. Consent management and data sharing restrictions
Patient consent adds a layer of legal and operational complexity to health information exchange that many teams underestimate during the design phase. Managing consent correctly means more than collecting a signature. It means tracking what each patient authorized, under what conditions, and ensuring your data flows respect those boundaries at runtime.
What this challenge looks like
Your application pulls records for a patient who previously opted out of data sharing for behavioral health information. The system sends that data anyway because consent preferences aren't encoded in the query parameters or enforced at the API level. This is one of the more consequential health information exchange challenges because violations aren't always visible until a patient or regulator flags them.
Why it happens
Consent frameworks vary significantly across state laws, federal regulations like 42 CFR Part 2, and individual health system policies. No single consent model applies universally, so teams often build generic flows that satisfy the most basic requirements while leaving edge cases unhandled. The result is a system that handles standard authorization correctly but fails on restricted data categories that carry heightened legal protections.
Behavioral health, substance use, and HIV-related data carry stricter consent requirements than general medical records, and treating them identically creates direct legal exposure.
How to overcome it
Build granular consent enforcement into your data pipeline at the resource level, not just the access layer. Map each data category to its applicable consent rules, and automatically filter or flag restricted data types before they leave your integration layer rather than relying on downstream applications to catch them.
Metrics to track
- Consent preference sync rate across connected EHRs
- Restricted data exposure incidents per quarter
- Consent verification failures at the point of data request
8. Governance, legal risk, and sustainability hurdles
Governance problems don't announce themselves loudly. They accumulate quietly through unclear data ownership, undefined roles, and agreements that no longer reflect how your integration actually operates. For many teams, governance and legal exposure represent the final layer of health information exchange challenges that surface only when something goes wrong.
What this challenge looks like
Your integration is live, but no one owns the decision about what happens when a data sharing partner changes their access policy or exits the relationship entirely. Data use agreements signed at project kickoff no longer match your current data flows, and your team has no documented process for reviewing them.
Why it happens
Governance structures are rarely prioritized during the build phase when speed to launch drives every decision. Legal agreements get drafted once and forgotten, and the gap between what those documents say and what your systems actually do widens with every new EHR connection you add.
The cost of fixing a governance gap after a regulatory review is almost always higher than the cost of building the right structure from the start.
How to overcome it
Assign explicit data stewardship roles within your organization and schedule annual reviews of every active data use agreement. Build a living data flow inventory that maps each integration, its legal basis, and its responsible owner so you can respond quickly when policies change.
Metrics to track
- Data use agreements reviewed on schedule per year
- Integrations without a named data steward at any given time
- Days to resolve a governance escalation from detection to closure
Next steps
The eight health information exchange challenges covered in this article share a common thread: each one compounds the others. Fragmented data models make identity matching harder. Poor consent enforcement creates governance gaps. Security gaps amplify audit risk. Tackling these problems in isolation rarely works, and rebuilding integration infrastructure from scratch pulls your team away from the work that actually delivers value to patients and care teams.
Your fastest path forward is to stop treating integration as a core engineering problem and start treating it as a solved one. Pre-built connectors, automated compliance, and a unified API remove the majority of the friction described in this article before your team writes a single line of application code. If you're ready to cut your integration timeline from months to days, launch your SMART on FHIR app with SoFaaS and see how much faster you can move when the infrastructure is already handled.
The Future of Patient Logistics
Exploring the future of all things related to patient logistics, technology and how AI is going to re-shape the way we deliver care.
Thank you! Your submission has been received!
Oops! Something went wrong while submitting the form.