Health Information Exchange Benefits: What You Gain From HIE

Patient data still gets stuck in silos. A home health agency faxes records to a hospital. A NEMT provider can't confirm eligibility without a phone call. Every one of these gaps costs time, money, and sometimes patient safety. Understanding health information exchange benefits matters because HIE is the infrastructure that closes those gaps, letting authorized systems share clinical data the moment it's needed instead of days later.
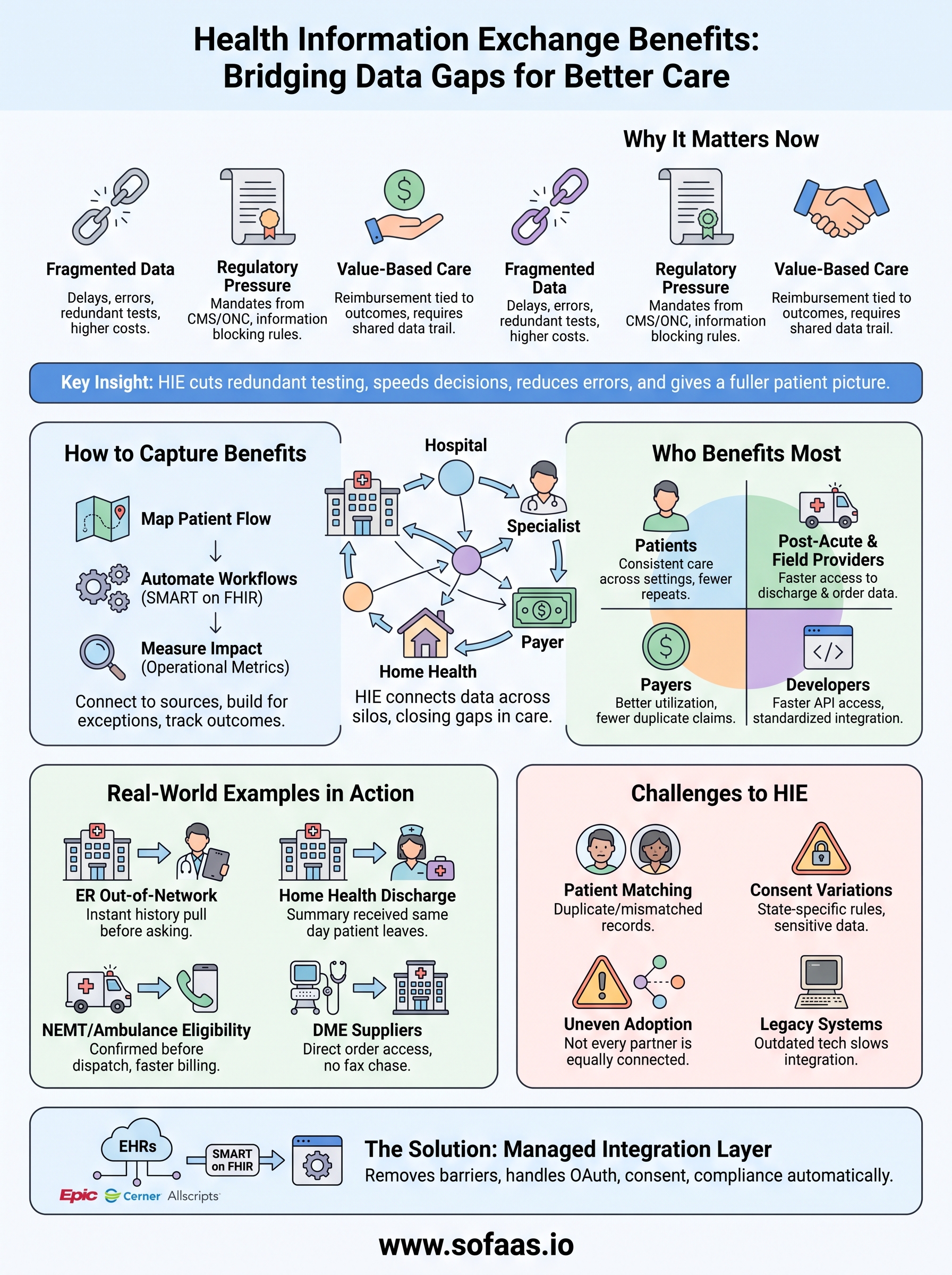
The short answer: HIE cuts redundant testing, speeds up care decisions, reduces medical errors from missing history, and gives providers a fuller picture of the patient in front of them. For healthcare organizations, it also means fewer manual data requests and lower administrative overhead. For patients, it means their record follows them, whether they're seen at an ER, a specialist's office, or a home health visit.
This article breaks down exactly what you gain from HIE, for patients, providers, and the broader healthcare system, and where the real value shows up in daily operations. If you're building or integrating an application that depends on this kind of data flow, you'll also see why standards like SMART on FHIR are what make these exchanges actually work in practice, not just in theory.
Why health information exchange benefits matter now
Healthcare data volume has exploded, but the systems moving that data haven't kept pace. Interoperability mandates from CMS and ONC have pushed hospitals, payers, and post-acute providers to open up data access, yet most organizations still rely on fax machines, portals that don't talk to each other, or phone calls to confirm basic patient information. The gap between what technology can do and what actually happens in daily practice is exactly where health information exchange benefits start to matter, because HIE closes that gap without requiring every provider to build custom integrations with every other provider.
The cost of fragmented data is no longer hidden
Government agencies have started putting numbers on what fragmentation actually costs. The Office of the National Coordinator for Health IT has documented how missing records drive duplicate testing, delayed diagnoses, and preventable readmissions, particularly for patients who move between hospitals, specialists, and home-based care. A home health nurse without visibility into a recent hospital discharge summary is flying blind. A DME supplier without access to a physician's order history has to chase down paperwork that already exists somewhere in the system. None of this is new, but the tolerance for it is shrinking as value-based care contracts tie reimbursement directly to outcomes and readmission rates.
When a provider can't see a patient's full history, the patient pays for it in delays, repeat tests, and avoidable errors.
Regulatory pressure is forcing the issue
Federal rules have moved from encouraging data sharing to requiring it. The 21st Century Cures Act's information blocking provisions, enforced by the Office of the National Coordinator for Health IT, make it a compliance violation for many healthcare entities to unreasonably withhold patient data from authorized requesters. That single shift changed the calculus for a lot of organizations that previously treated data sharing as optional or a competitive disadvantage. Now it's a legal expectation, and the organizations that build real exchange capability instead of just checking a compliance box are the ones capturing the operational upside alongside the legal cover.
Smaller and mid-size providers finally have a path in
For years, real-time data exchange was mostly a large-hospital-system advantage. Building direct interfaces to Epic, Cerner, or Allscripts took integration teams, months of work, and ongoing maintenance that smaller organizations couldn't justify. That's changed. Managed platforms and standardized APIs have lowered the barrier enough that a NEMT provider, an ambulance service, or a home health agency can plug into the same data streams that used to be reserved for large health systems.
| Era | Typical data access method | Time to connect |
|---|---|---|
| Pre-2015 | Fax, phone, manual chart requests | Days to weeks |
| 2015 to 2020 | Custom point-to-point interfaces | Months, per connection |
| 2020 to present | Standardized APIs (SMART on FHIR), HIE networks | Days |
Patient expectations have shifted too
Finally, patients themselves expect their data to move. Someone who gets a prescription filled, sees a specialist, and visits an urgent care clinic in the same month assumes those providers can see each other's notes. When they can't, and a patient has to re-explain their medication list for the third time in a week, it erodes trust in the whole system. That expectation is part of why interoperability has become a strategic priority rather than a back-office IT project. Organizations that treat HIE as core infrastructure, not an optional add-on, are the ones positioned to meet both the regulatory bar and the expectations of the people they serve.
How to capture the benefits of health information exchange
Access to a network doesn't automatically translate into value. Plenty of organizations connect to an HIE and still operate the old way, because the data never reaches the workflow where a decision actually gets made. Capturing real health information exchange benefits takes a deliberate setup: the right connections, a plan for exceptions, and a way to measure whether anything actually changed.
Connect to the sources that match your patient flow
Before anything else, map where your patients actually come from and go to. A home health agency needs discharge summaries from local hospitals more than it needs specialist notes from across the state. An ambulance service needs eligibility and medication history at the point of dispatch, not after the fact. Prioritizing connections by actual patient volume, rather than trying to integrate with every EHR at once, gets you usable data faster and avoids burning budget on integrations that rarely get used.
Build workflows around exceptions, not just clean data
Data that arrives late, incomplete, or duplicated is the norm, not the exception, so your workflow has to plan for it. Teams that treat every exchange as a perfect handoff end up frustrated the first time a record doesn't match or a patient has two different identifiers across systems.
- Set a rule for what happens when a query returns no data
- Flag duplicate patient records for manual review instead of silently merging them
- Log every failed or delayed exchange so patterns show up over time
- Assign an owner for resolving mismatched or incomplete records
The benefit isn't the data feed itself, it's what your team does with the data once it arrives.
Automate the parts that don't need a human
Getting a real return from HIE also means removing the manual steps that used to justify a staff member's time. Authorization checks, consent management, and token refreshes are exactly the kind of repetitive work that should run in the background instead of sitting in someone's inbox. This is where a managed integration layer built on SMART on FHIR earns its keep, because it handles OAuth flows and connection maintenance automatically instead of requiring an internal team to babysit every EHR connector.
Measure the operational impact, not just the connection count
Having five EHR connections live means nothing if nobody tracks what changed downstream. Metrics worth watching include time to retrieve a record, number of duplicate tests avoided, and reduction in phone calls to confirm patient information. Reviewing these numbers quarterly gives you a clear signal about whether your integration strategy is actually paying off or just adding technical overhead. Organizations that track this closely tend to expand their exchange capability deliberately, connection by connection, rather than chasing every available network at once.
Who benefits most from health information exchange
Not every stakeholder gains the same amount from health information exchange benefits, and understanding who gets the most out of it helps you prioritize where to invest. Patients, frontline providers, payers, and the developers building the tools that connect everyone all see different slices of the value, but the biggest gains tend to land with the people making time-sensitive decisions with incomplete information.
Patients moving between care settings
People with chronic conditions, recent hospital discharges, or multiple specialists on their care team benefit the most directly, because their history is scattered across the most systems. A patient discharged after a cardiac event who then sees a home health nurse, a cardiologist, and a primary care doctor within two weeks needs every one of those providers working from the same medication list and discharge instructions. Without exchange, that patient repeats their story at every stop and absorbs the risk when something gets missed.

The patients with the most complex care journeys have the most to lose when their data doesn't travel with them.
Post-acute and field-based providers
Home health agencies, DME suppliers, ambulance services, and NEMT providers historically sat at the edge of the data flow, often the last to receive information that hospitals and large clinics shared freely among themselves. These organizations gain outsized value from HIE because their staff work outside a hospital's four walls, without easy access to a shared chart, so a real-time feed of eligibility, orders, and clinical history replaces phone tag and faxed paperwork.
| Stakeholder | Primary HIE benefit |
|---|---|
| Patients | Fewer repeated tests, consistent care across settings |
| Home health & post-acute providers | Faster access to discharge and order data |
| Payers | Better utilization data, fewer duplicate claims |
| Health tech developers | Faster, standardized access to EHR data via APIs |
Payers and value-based care organizations
Insurers and accountable care organizations benefit from HIE in a less visible but financially significant way. Complete data means fewer duplicate claims, better risk adjustment accuracy, and clearer visibility into whether a patient actually received the follow-up care a treatment plan called for. Value-based contracts depend on this kind of visibility, since reimbursement is tied to outcomes that are hard to verify without a shared data trail.
Developers and product teams building on top of EHR data
Software teams building healthcare applications gain something more practical: a shorter path from idea to working product. Instead of negotiating custom interfaces with every EHR vendor, teams that build on standards like SMART on FHIR inherit the connections and consent flows that HIE infrastructure already handles, which turns a months-long integration project into a matter of days.
Real-world examples of HIE benefits in action
Abstract benefits are easy to state and hard to picture, so it helps to walk through what actually happens when the data moves correctly. Each of these scenarios reflects the kind of exchange that healthcare suppliers encounter daily, not a hypothetical future state.
An emergency department pulling up out-of-network history
Consider a patient who collapses while traveling and is brought to an ER where they've never been seen before. Without exchange, the care team starts from zero: no medication list, no allergy history, no record of the cardiac stent placed six months earlier at a different hospital system. With an active HIE connection, that ER pulls the patient's history from a regional network within seconds of registration. The Centers for Medicare & Medicaid Services has pointed to exactly this kind of scenario as a driver behind its interoperability rules, because the alternative is a physician making treatment decisions blind.

A patient's history showing up before the doctor asks for it is the clearest sign HIE is working as intended.
Home health agencies receiving discharge summaries automatically
Discharge day used to mean a home health nurse waiting on a fax that might arrive hours or days late, if it arrived at all. Agencies connected to a hospital's exchange network now receive the discharge summary, medication reconciliation, and physician orders the same day the patient leaves the hospital. That timing difference matters clinically: a nurse walking into a first home visit with accurate medication information catches dosing conflicts before they become a readmission.
Ambulance and NEMT providers confirming eligibility in real time
Field-based transport providers historically confirmed patient eligibility over the phone, often after a trip had already happened. Real-time exchange changes that sequence entirely.
- Eligibility and coverage status confirmed before dispatch, not after
- Recent diagnosis codes available to inform the level of transport needed
- Fewer denied claims tied to missing or outdated patient information
- Faster billing cycles because documentation doesn't need to be chased down after the fact
DME suppliers cutting the paperwork chase
Durable medical equipment suppliers spend a disproportionate amount of staff time tracking down physician orders and supporting documentation that already exists somewhere in the health system. Suppliers with direct access to a patient's order history through an EHR-connected exchange skip the fax-and-follow-up cycle entirely. Instead of a staff member calling three different clinics to locate a signed order, the documentation is already sitting in the workflow, verified and ready for a claim. That single change often shortens the time between a physician's order and equipment delivery from weeks to days, which is the kind of measurable outcome that justifies the integration in the first place.
Challenges that can limit health information exchange benefits
Even with strong infrastructure in place, real barriers keep organizations from capturing the full value of health information exchange benefits. Recognizing these obstacles early lets you plan around them instead of discovering them mid-project.
Patient matching still breaks down
Duplicate and mismatched patient records remain one of the most persistent problems in HIE. Two systems using different identifiers for the same person can create split records, meaning a provider pulling history might see only half the picture without realizing anything is missing. The ONC has flagged patient matching as a top-tier interoperability problem for years, and it hasn't fully resolved because no national patient identifier exists in the US.
A missing record is obvious. A mismatched one is dangerous, because nobody knows it's wrong.
Consent rules vary by state and data type
Behavioral health, substance use treatment, and reproductive health records often carry stricter consent requirements than general medical data, and those rules differ from state to state. An exchange network built for standard clinical data can stall completely when it hits a record type that needs separate authorization. Teams that don't account for this upfront end up with gaps in exactly the records where continuity of care matters most.
Not every partner is equally connected
HIE only delivers value when the organizations on both ends participate meaningfully, and adoption is still uneven.
- Large hospital systems often connect early, while smaller clinics lag behind
- Rural providers may lack the bandwidth or IT staff to maintain a connection
- Some EHR vendors historically restricted data access to protect market position
- Specialty practices sometimes skip exchange participation entirely, leaving gaps in a patient's record
Each gap in the network becomes a blind spot for anyone downstream trying to build a complete patient picture.
Legacy systems slow everything down
Older EHR installations and homegrown practice management systems weren't built with modern APIs in mind, and retrofitting them for real-time exchange can be expensive and slow. Organizations stuck on outdated infrastructure often fall back on batch file transfers or manual exports, which undercuts the real-time advantage that makes HIE valuable in the first place. This is precisely where a managed integration layer pays for itself, since it absorbs the complexity of connecting to inconsistent, legacy-heavy environments instead of leaving each organization to solve that problem on its own. Working around these gaps, rather than ignoring them, is what separates organizations that get real value from HIE from those that just have a connection sitting unused.
The bottom line on HIE benefits
Health information exchange benefits show up wherever a decision depends on data that used to sit in another system. Patients get consistent care across settings, providers spend less time chasing paperwork, and payers get cleaner claims. None of that happens automatically. It takes real connections to the right sources, workflows built for messy data, and infrastructure that handles authorization and compliance without a team babysitting it full time.
That last part is where most organizations get stuck. Building SMART on FHIR connections to Epic, Cerner, or Allscripts from scratch takes months and specialized expertise most teams don't have on staff. A managed integration layer removes that barrier entirely, handling OAuth, consent, and compliance so your team can focus on the application itself instead of the plumbing underneath it.
If you're ready to connect your application to EHR data without building that infrastructure yourself, launch your SMART on FHIR app in a couple of steps.
The Future of Patient Logistics
Exploring the future of all things related to patient logistics, technology and how AI is going to re-shape the way we deliver care.
Thank you! Your submission has been received!
Oops! Something went wrong while submitting the form.