mTLS vs OAuth: Differences, Use Cases, And When To Use Both

Security in healthcare integration isn't a single-layer problem. When you're connecting applications to EHR systems, you need to get both authentication and authorization right, and that means understanding the tools available. The mTLS vs OAuth debate comes up constantly in architecture discussions, especially when teams are designing machine-to-machine communication pipelines that handle sensitive patient data.
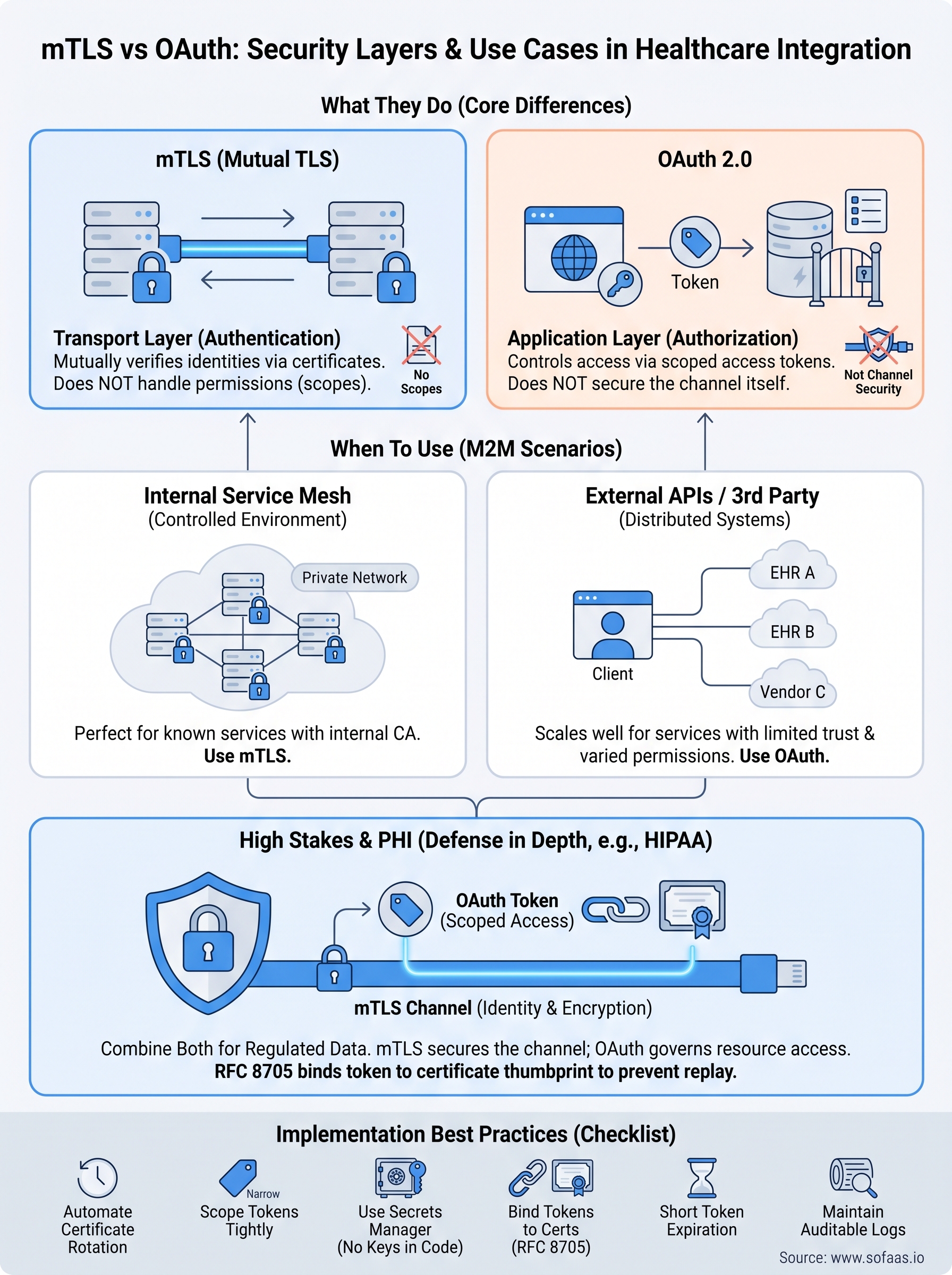
Here's the short version: mTLS and OAuth solve different problems at different layers of the security stack. mTLS verifies that both ends of a connection are who they claim to be using mutual certificate exchange. OAuth controls what an authenticated party is actually allowed to do once that connection is established. They're not interchangeable, but they're not mutually exclusive either.
At SoFaaS, we deal with this firsthand. Our managed SMART on FHIR platform handles OAuth authorization flows for EHR integrations across Epic, Cerner, Allscripts, and others, so healthcare application teams don't have to build and maintain that infrastructure themselves. We've seen how often teams conflate these two protocols or underestimate the complexity of implementing them correctly in a healthcare context.
This article breaks down the core differences between mTLS and OAuth, walks through their respective use cases, and explains when you should use one, the other, or both together. By the end, you'll have a clear framework for making that architectural decision with confidence.
What mTLS and OAuth do and do not do
Understanding these two protocols requires separating the concepts of authentication and authorization. They're often treated as synonyms in casual conversation, but in security architecture they describe distinct processes. mTLS handles the first: proving identity at the transport layer. OAuth handles the second: controlling access to resources once identity is established. When teams confuse the two, they end up with systems that are either over-engineered in one area or dangerously unprotected in another.
What mTLS does (and doesn't)
Mutual TLS (mTLS) is an extension of standard TLS, the protocol that secures HTTPS connections. In a standard TLS handshake, only the server presents a certificate and the client verifies it. mTLS changes that: both the client and the server present certificates, and both parties verify each other before any data moves across the wire. This mutual verification happens at the network transport layer, before your application code ever runs.
mTLS confirms that a connection is between two trusted parties, but it says nothing about what those parties are permitted to do once connected.
What mTLS does not do is carry any concept of scopes, permissions, or resource-level access control. A certificate either passes verification or it doesn't. If a client certificate passes, that client gets a raw authenticated connection. There's no built-in mechanism for saying "this client can read patient records but cannot write them." You'd have to build that logic yourself on top of the transport layer, which quickly becomes custom, difficult to maintain, and hard to audit at scale.
What OAuth does (and doesn't)
OAuth 2.0 is an authorization framework, not an authentication protocol. It provides a standardized way for an application to obtain limited access to a resource on behalf of a user or service account. The framework issues access tokens with defined scopes, so a client can request exactly the permissions it needs, and the resource server can enforce those boundaries on every request without building custom permission logic from scratch.
What OAuth does not do is secure the transport channel itself. OAuth tokens travel over HTTPS, meaning you rely on standard TLS to protect them in transit. If a token gets intercepted, an attacker can replay it until it expires. OAuth provides no native mechanism for verifying that the client sending a token is the same party that originally received it, unless you layer in an explicit binding mechanism like DPoP or certificate-bound access tokens.
This is where the mTLS vs OAuth comparison becomes genuinely useful rather than academic. Each protocol has a structural gap that the other fills directly. mTLS secures the channel and binds identity to the connection itself; OAuth carries structured authorization data and enforces granular access control at the application layer. Neither one alone gives you a complete security model for high-stakes integrations, particularly in healthcare environments where both channel security and fine-grained data access controls are regulatory requirements, not optional features.
mTLS vs OAuth in machine-to-machine APIs
Machine-to-machine (M2M) communication presents a specific security challenge: there's no human user to log in, enter a password, or approve an OAuth consent screen. Services call other services directly, often thousands of times per minute. In that environment, the mTLS vs OAuth decision becomes a core architectural question rather than a secondary concern.
How mTLS secures M2M connections
In a pure M2M context, mTLS is a natural fit for establishing trusted connections between known services. When a backend service calls another internal service, both sides present certificates issued by a shared certificate authority (CA). If either certificate fails validation, the connection terminates before any payload is sent. This model works well for service meshes and private API networks where you control both ends of every connection and can manage certificate lifecycle systematically.
The limitation surfaces when you need to call external APIs or manage access for third-party services that you don't provision yourself.
Outside that controlled environment, distributing and rotating certificates across services you don't fully control creates operational complexity that compounds quickly.
How OAuth handles M2M authorization
For M2M scenarios, OAuth 2.0 provides the Client Credentials grant, which allows a service to authenticate directly with an authorization server using a client ID and secret, then receive an access token with defined scopes. This removes the need for user-delegated consent and still enforces precise resource-level permissions. The authorization server issues short-lived tokens, and your downstream APIs validate those tokens on every request without needing to know anything about how the calling service authenticates itself.
This token-based approach scales much more cleanly across distributed systems and third-party integrations than certificate management does. You can issue tokens with narrow scopes, revoke them instantly, and audit them per request. For healthcare applications connecting to EHR systems through standards like SMART on FHIR, OAuth's Client Credentials flow is the mechanism that governs what data a backend service can actually retrieve, regardless of how the underlying connection is secured.
When to use mTLS, OAuth, or both
The mTLS vs OAuth decision isn't always binary. Your architecture, threat model, and integration context all shape which protocol belongs where. The clearest way to approach this is to match each protocol to the security problem it actually solves, rather than defaulting to one because it feels more familiar.
Use mTLS when you control both ends
mTLS makes the most sense when you operate a private service mesh or internal API network where you provision and rotate certificates for every service involved. If your backend services live inside a controlled infrastructure, like a Kubernetes cluster or a private cloud VPC, mTLS gives you strong mutual authentication at the network layer with minimal runtime overhead. Internal healthcare data pipelines, for example, benefit from this model because you own both sides of every connection and can enforce certificate policies systematically.
The moment you need to integrate with external systems or third-party vendors, certificate-based identity management gets complicated fast.
Use OAuth when you need granular access control
OAuth is the right choice when your application needs to request specific permissions against an external API, or when a backend service needs to call a resource server without user involvement. Healthcare applications connecting to EHR systems through SMART on FHIR rely on OAuth's Client Credentials flow precisely because it lets you define narrow, auditable scopes for exactly what data your service can access. Tokens are short-lived, revocable, and carry structured claims that resource servers can verify without any shared secret or certificate infrastructure.
Use both when the stakes are high
For healthcare integrations handling Protected Health Information (PHI), using mTLS and OAuth together gives you defense in depth. OAuth governs what your application can access at the resource level. mTLS ensures the token itself only travels over a connection between verified parties, eliminating token replay risk. Regulated environments like those governed by HIPAA benefit directly from this layered approach, because it addresses both transport-layer identity and application-layer authorization without leaving either gap open.
How to combine OAuth with mTLS safely
Combining mTLS and OAuth in the same system isn't complicated in concept, but the implementation details matter. The goal is to bind an OAuth access token to the client certificate that was used during the TLS handshake, so that even if a token leaks, no other party can use it without presenting the matching certificate. RFC 8705 defines exactly this mechanism, known as OAuth 2.0 Mutual-TLS Client Authentication and Certificate-Bound Access Tokens, and it's the right starting point for any team taking this approach seriously.
Bind tokens to certificates
The core technique involves configuring your authorization server to embed a certificate thumbprint (a SHA-256 hash of the client certificate's public key) inside the access token itself. When a resource server receives that token, it verifies the thumbprint against the certificate presented in the mTLS connection. If they don't match, the request fails, regardless of whether the token is otherwise valid. This eliminates replay attacks entirely because a stolen token carries no value without the corresponding private key.

Binding tokens to certificates transforms OAuth from a bearer-token model into a possession-based model, which directly addresses the biggest vulnerability in standard OAuth deployments.
Your authorization server needs explicit support for this. Both Microsoft Entra ID and major identity platforms expose configuration options for mTLS client authentication, so check your provider's documentation before building any custom logic on top.
Scope tokens tightly at issuance
Even with mTLS binding in place, you should still issue tokens with the narrowest scopes possible for each service. Certificate binding prevents replay, but it doesn't limit what an authenticated client can do once connected. For healthcare applications that handle PHI under HIPAA, tight scoping means a compromised service can only access the data it was explicitly authorized to retrieve, not everything your integration touches. When you think about mTLS vs OAuth as a combined system, certificate binding handles transport identity and token scoping handles resource-level containment. Both layers need deliberate configuration to work correctly.
Common pitfalls and a security checklist
Even teams that understand the mTLS vs OAuth distinction at a conceptual level run into problems during implementation. The most common mistakes don't come from misunderstanding the protocols themselves; they come from misconfiguring the details or making assumptions that hold up in development but fail in production. Knowing where these gaps typically appear lets you avoid them before they become security incidents.
Pitfalls to avoid
The first pitfall is treating certificate expiration as a low-priority operational task. In mTLS deployments, an expired certificate causes an immediate and complete connection failure. Teams that don't automate certificate rotation end up scrambling to restore connectivity during incidents, often under pressure to skip validation steps. Build automated rotation into your certificate lifecycle from day one, not after your first outage.
Token scope creep is the OAuth equivalent of this problem: access tokens that started narrow gradually accumulate permissions as features get added, until a compromised token exposes far more than it should.
The second pitfall is storing client secrets or private keys in source code or environment files that get committed to version control. Both OAuth client credentials and mTLS private keys need to be managed through a dedicated secrets manager. If your private key leaks, an attacker can impersonate your service entirely, regardless of how well your token scoping is configured.
Security checklist
Use the checklist below to verify your implementation covers the critical bases before you move any PHI or sensitive healthcare data through your integration.
- mTLS certificates are issued by a controlled internal CA, not self-signed
- Certificate expiration and automated rotation are monitored in production
- OAuth tokens use the narrowest possible scopes for each service
- Client secrets and private keys are stored in a secrets manager, not in code or config files
- Access tokens are certificate-bound via RFC 8705 if you're combining both protocols
- Token expiration windows are short-lived (15 minutes or less for sensitive resources)
- Authorization server logs are retained and auditable for compliance purposes
Next steps
The mTLS vs OAuth comparison comes down to a straightforward principle: use mTLS to secure the channel, use OAuth to control what flows through it, and combine both when your data carries real risk. For healthcare applications handling PHI under HIPAA, that combination isn't optional. It's the architecture that regulators, auditors, and security teams expect to see.
If your team is building a healthcare application that needs to connect to Epic, Cerner, or Allscripts, the OAuth side of this equation, specifically the SMART on FHIR authorization flows, is the part that takes the most time to implement correctly. Certificate management is operational work you can systematize. Getting EHR authorization flows right requires deep familiarity with healthcare-specific OAuth profiles, token scoping rules, and EHR vendor configurations.
SoFaaS handles that complexity for you so your team can focus on the application itself. Connect your app to EHR systems in days, not months.
The Future of Patient Logistics
Exploring the future of all things related to patient logistics, technology and how AI is going to re-shape the way we deliver care.
Thank you! Your submission has been received!
Oops! Something went wrong while submitting the form.